



Peritoneum, structure, functions
Peritoneum, peritoneum, - a thin serous membrane with a smooth, shiny, uniform surface, covers the walls of the abdominal cavity, cavitas abdominis, and partly the small pelvis located in this cavity of organs. The surface of the peritoneum is about 20 400 cm 2 and is almost equal to the skin area. Peritoneum form their own plate, lamina propria, serosa and covering its single-layered flat epithelium - mesothelium, mesothelium.
The peritoneum that lines the abdominal wall is called the parietal peritoneum, peritoneum parietale; The peritoneum covering the organs, - the visceral peritoneum, peritoneum viscerale. Passing from the walls of the abdominal cavity to the organs and from one organ to the other, the peritoneum forms ligaments, ligamenta, folds, plicae, mesentery, mesenterii.
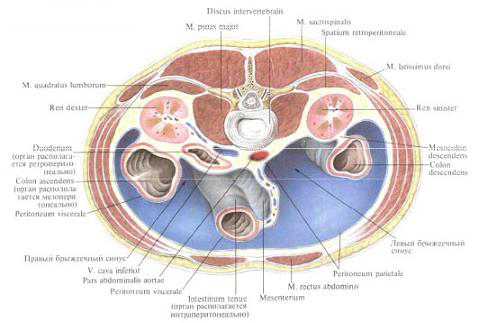
Due to the fact that the visceral peritoneum covering this or that organ passes into the peritoneal peritoneum, most organs are fixed to the walls of the abdominal cavity. The visceral peritoneum covers organs differently: from all sides (intraperitoneally), from three sides (mesoperitoneally) or from one side (retro- or extraperitoneally). To the organs covered by the peritoneum on three sides, located mesoperitoneally, are the liver , gall bladder , partially ascending and descending parts of the colon , the middle part of the rectum .
To the extraperitoneally located organs are the duodenum (except its initial section), pancreas, kidneys , adrenals, ureters .
The organs located intraperitoneally have a mesentery connecting them with the parietal peritoneum .
Mesentery is a plate consisting of two connected sheets of the peritoneum of the duplication. One - free - the edge of the mesentery covers the organ (gut), as if hanging it, and the other edge goes to the abdominal wall, where its leaves diverge in different directions in the form of a parietal peritoneum. Usually between the leaves of the mesentery (or ligament) to the body fit blood, lymph vessels and nerves. The place of the beginning of the mesentery on the abdominal wall is called the mesentery root, radix mesenterii; Going to the organ (for example, to the gut), its leaves diverge on both sides, leaving a narrow strip near the attachment site - the extraperitoneal field, area nuda.
The serosa, or serosa, tunica serosa, does not directly adhere to the organ or abdominal wall, but is separated from them by a layer of connective tissue undernearth base, tela subserosa, which, depending on the location, has a different degree of development. Thus, the under-serous base under the serous membrane of the liver, the diaphragm, the upper part of the anterior wall of the abdomen and, on the contrary, is considerably developed under the parietal peritoneum lining the posterior wall of the abdominal cavity; For example, in the area of the kidneys, etc., where the peritoneum is very mobilely connected to the underlying organs or parts thereof.
The peritoneal cavity, or cavity of the peritoneum, cavitas peritonealis, is closed in men, and in women through the fallopian tubes, uterus and vagina communicates with the external environment. The cavity of the peritoneum is a slotted space of complex shape, filled with a small amount of serous fluid, liquor peritonei, moisturizing surface of the organs.
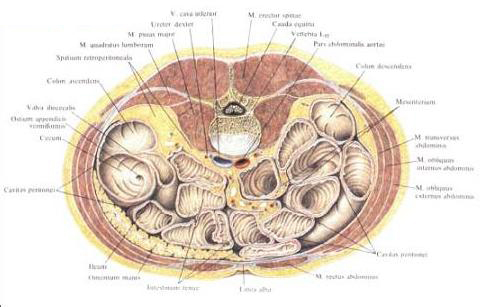
The parietal peritoneum of the posterior wall of the abdominal cavity delimits the peritoneal cavity from the retroperitoneal space, the spatium retroperitoneale, in which the retroperitoneal organs lie, organa retroperitonealia. In retroperitoneal space, behind the parietal peritoneum, is the retroperitoneal fascia, fascia retroperitonealis.
The extraperitoneal space, spatium extraperitoneale, is also the phallus space, the spatium retropubicum.
Peritoneum and peritoneal folds. The anterior parietal peritoneum, peritoneum parietale anterius, forms a series of folds on the anterior wall of the abdomen. On the middle line is the middle umbilical fold, plica umbilicalis mediana, which extends from the umbilical ring to the tip of the bladder ; In this fold a connective tissue lining is formed, which is an obliterated urinary duct, the urachus. From the umbilical ring to the lateral walls of the bladder, there are medial umbilical folds, plicae umbilicales mediales, in which tendons of empty front sections of umbilical arteries are laid. Outside these folds are lateral umbilical folds, plicae umbilicales laterales. They stretch from the middle of the inguinal ligament obliquely up and down, to the back wall of the vagina of the rectus abdominal muscles . These folds contain the lower epigastric arteries, aa. Epigastricae inferiores, which feed the rectus abdominis muscles.
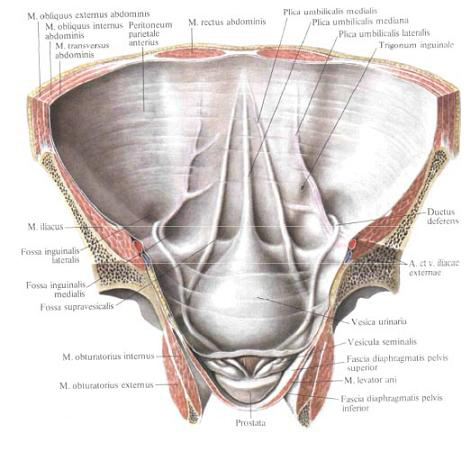
At the base of these folds pits are formed. On both sides of the median umbilical fold, between it and the medial umbilical fold, above the upper edge of the bladder, there are nasepuzyr pits, fossae supravesicales. Between the medial and lateral umbilical folds are medial inguinal pits, fossae inguinales mediates; Outside the lateral umbilical folds lie lateral inguinal fossae, fossae inguinales laterales; These pits are located opposite the deep inguinal rings.
The triangular part of the peritoneum, located above the medial inguinal fossa and bounded from the medial side by the edge of the rectus abdominal muscle, with the lateral - lateral umbilical fold and from below - the inner part of the inguinal ligament, is called the inguinal triangle, trigonum inguinale.
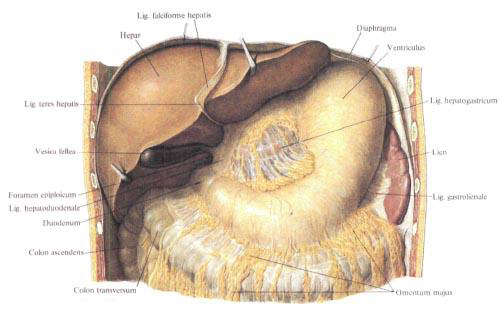
The parietal peritoneum, covering the abdominal forearm above the umbilical ring and the diaphragm, passing to the diaphragmatic surface of the liver, forms a crescent (suspending) ligamentous ligament. Falciforme hepatis, consisting of two sheets of peritoneum (duplication), located in the sagittal plane. In the free lower edge of the crescent ligament passes the ligaments of the circular ligament of the liver, lig, teres hepatis. The leaves of the crescent ligament posteriorly pass into the front sheet of the coronary ligament of the liver, lig. Coronarium hepatis. It represents the transition of the visceral peritoneum to the diaphragmatic surface of the liver into the parietal peritoneum of the diaphragm. The posterior leaf of this ligament passes to the diaphragm from the visceral surface of the liver. Both sheets of the coronary ligament meet laterally and form a right and left triangular ligament, lig. Triangulare dextrum et lig. Triangulare sinistrum.
The visceral peritoneum, peritoneum visceralis, of the liver covers the gallbladder from the lower side.
From the visceral peritoneum of the liver is directed the peritoneal ligament to the small curvature of the stomach and the upper part of the duodenum. It is a duplicate of the peritoneal sheet starting from the edges of the gate (transverse furrow) and from the edges of the venous ligament slit, and is located in the frontal plane. The left part of this ligament (from the slit of the venous ligament) goes to a small curvature of the stomach - a hepatic-gastric ligament, lig, hepatogastricum. It looks like a thin cobweb-like plate. Between the sheets of the hepatic-gastric ligament, along the small curvature of the stomach, pass the arteries and veins of the stomach, a. Et v. Gastricae, nerves; There are regional lymph nodes. The right part of the ligament, more dense, goes from the liver gate to the upper edge of the pylorus and duodenum, this section is called the hepatic duodenal ligament, lig. Hepatoduodenale, and includes a common bile duct, a common hepatic artery and its branches, a portal vein, lymphatic vessels, nodes and nerves. On the right, the hepatic-duodenal ligament forms the leading edge of the gland opening, foramen epiploicum (omentale). Going to the edge of the stomach and duodenum, the ligament leaves diverge and cover the front and back walls of these organs.
Both ligaments: hepatic-gastric and hepatic-duodenal - make up a small omentum, omentum minus. The inconsistent continuation of the small omentum is the hepatic-ligament ligament, lig. Hepatocolicum, connecting the gallbladder with the duodenum and right bend of the colon. Sickle ligament and small omentum are ontogenetically anterior, ventral, mesentery of the stomach.
From the left side of the dome of the diaphragm, the parietal peritoneum, passing to the cardial notch and the right half of the arch of the stomach, forms a small gastro-diaphragmatic ligament, lig. Gastrophrenicum.
Between the lower edge of the right lobe of the liver and the upper end of the right kidney attached here, the peritoneum forms a transitional fold - the hepatic-renal ligament, lig. Hepatorenale.
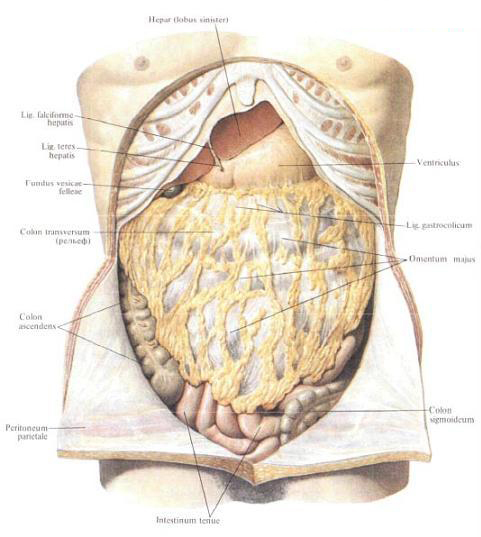
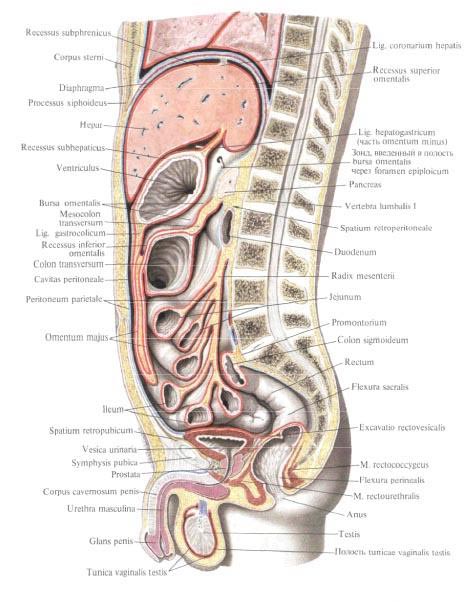
The leaves of the visceral peritoneum of the anterior and posterior surfaces of the stomach, along a large curvature of it, continue downward as a large omentum. A large omentum, omentum majus, in the form of a wide plate ("apron") should be down to the level of the upper aperture of the small pelvis. Here, the two sheets forming it turn and return, going upward behind the downward two sheets. These return sheets are spliced with the front sheets. At the level of the transverse colon all four leaves of the large omentum grow to the glandular tape located on the front surface of the intestine. Then the back (return) gland leaves move away from the forelegs, connect to the mesentery of the transverse colon, mesocolon transversum, and go together dorsally to the line of attachment of the mesentery to the posterior abdominal wall in the region of the anterior edge of the body of the pancreas.
Thus, a pocket is formed between the front and back sheets of the gland at the level of the transverse colon. Approaching the anterior edge of the body of the pancreas, the two posterior plates of the omentum diverge: the upper leaf passes into the back wall of the stuffing bag (on the surface of the pancreas) in the form of a parietal peritoneal sheet, the lower one passes into the upper sheet of the mesentery of the transverse colon.
The site of the large epiploon between the large curvature of the stomach and the transverse colon is called the gastric-ligament ligament, lig. Gastrocolicum; This ligament fixes the transverse colon to the large curvature of the stomach. Right and left gastro-omental arteries and veins pass through the leaves of the gastro-colonic ligament along the large curvature, regional lymph nodes overlap.
A large omentum covers the front of the thick and small intestine. Between the omentum and the anterior abdominal wall a narrow gap is formed - the pre-altitude space. The large omentum is a stretched dorsal mesentery of the stomach. Its continuation to the left is the gastro-splenic ligament, lig. Gastrolienale, and diaphragm-splenic ligament, lig. Phrenicolienale, which pass one into another.
Of two sheets of the peritoneum of the gastro-splenic ligament, the anterior passes to the spleen, surrounds it from all sides, returns back to the organ gates in the form of a leaf of the diaphragmatic-splenic ligament. The posterior sheet of the gastro-splenic ligament, reaching the spleen gates, turns directly to the posterior abdominal wall in the form of a second leaf of the diaphragmatic-splenic ligament. As a result, the spleen, as it were, is included laterally into the ligament, which connects the large curvature of the stomach with the diaphragm.
Mesentery of the colon, mesocolon, varies in different parts of the colon, and sometimes it is absent. So, the caecum, shaped like a sac, is covered with the peritoneum on all sides, but it does not have a mesentery. At the same time, the worm-like process leaving the cecum, surrounded also on all sides by the peritoneum (intraperitoneal position), has a mesenteric process, mesoappendix, reaching considerable dimensions. At the place of passage of the cecum into the ascending colon there is sometimes an insignificant mesentery of the ascending colon, mesocolon ascendens.
Thus, the serous shell covers the ascending colon on three sides, leaving the posterior wall free (mesoperitoneal position).
Mesentery of the transverse colon begins on the posterior abdominal wall at the level of the descending part of the duodenum, the head and body of the pancreas, the left kidney; Going to the intestine of the mesenteric tape, two sheets of mesentery diverge and cover the gut round (intraperitoneally). Throughout the mesentery from the root to the place of attachment to the intestine, its greatest width is 10-15 cm and decreases towards the bends, where it passes into the parietal leaf.
The descending colon, as well as the ascending one, is covered with a serous membrane from three sides (mesoperitoneally), and only in the area of transition to the sigmoid colon is a short mesentery of the descending colon, mesocolon descendens. It is covered with a peritoneum only a small portion of the posterior wall of the middle third of the descending colon.
The mesentery of the sigmoid colon, mesocolon sigmoideum, has a width of 12-14 cm, which varies considerably throughout the colon. The root of the mesentery crosses the iliac fossa obliquely to the left and top to the bottom and to the right, the iliac and lumbar muscles, and the left common iliac vessels and the left ureter located along the border line; Circling the boundary line, the mesentery crosses the region of the left sacroiliac joint and passes to the anterior surface of the superior sacral vertebrae. At level III of the sacral vertebra, the mesentery of the sigmoid colon terminates at the beginning of a very short mesentery of the rectum. The length of the mesentery root varies greatly; The steepness and size of the loop of the sigmoid colon depend on it.
The ratio of the rectum to the peritoneum of the small pelvis varies at different levels. The pelvic part is more or less covered with a serous membrane. The perineal part is devoid of peritoneal cover. The uppermost (namdapular) part, beginning at level III of the sacral vertebra, is completely surrounded by a serous cover and has a short and narrow mesentery.
The left flexure of the colon is connected to the diaphragm horizontally located by the peritoneal diaphragmatic-fold fold (sometimes referred to as the diaphragmatic ligament, lig. Phrenicocolicum).
For a more convenient study of the topography of the peritoneum and the organs of the abdominal cavity, a number of topographic and anatomical definitions used in the clinic and not having both Latin terms and their Russian equivalents are used.
Peritoneal folds, ligaments, mesentery and organs create in the cavity of the peritoneum relatively isolated grooves, pockets, bags and sinuses.
On this basis, the peritoneal cavity can be divided into the upper floor and the lower floor.
The upper floor is separated from the lower horizontal mesentery of the transverse colon (level II of the lumbar vertebra). The mesentery is the lower boundary of the upper floor, the diaphragm is the upper one, and the lateral walls of the abdominal cavity limit it on the sides.
The lower floor of the cavity of the peritoneum is bounded from above by the transverse colon and its mesentery, along the sides by the lateral walls of the abdominal cavity, at the bottom by the peritoneum covering the pelvic organs.
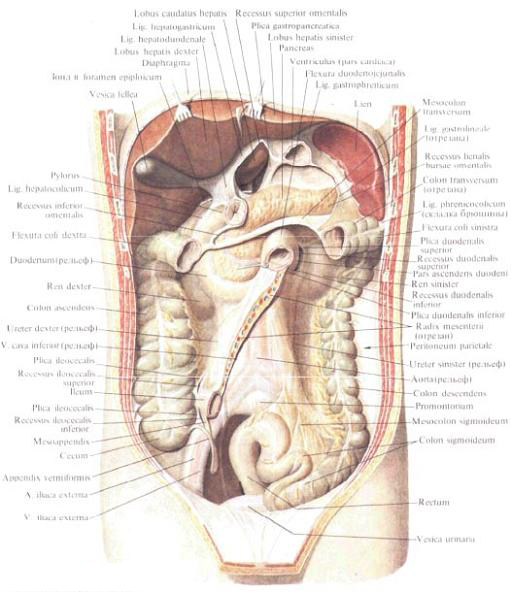
In the upper floor of the peritoneal cavity, subdiaphragmatic indentations are distinguished, recessus subphrenici, submental grooves, recessus subhepatici, and omentum bag, bursa omentalis.
Subdiaphragmatic recess with sickle ligament is divided into right and left parts. The right part of the sub-diaphragmatic depression is the gap of the peritoneal cavity between the diaphragm surface of the right lobe of the liver and the diaphragm. Behind it it is limited by the right part of the coronary ligament and by the right triangular ligament of the liver, to the left by the crescent ligament of the liver. This recess communicates with the lower right parietal space located below, the right peripheral-intestinal furrow, further with the ileum and through it with a small pelvis. The space under the left dome of the diaphragm between the left lobe of the liver (diaphragmatic surface) and the diaphragm is the left sub-diaphragmatic depression.
On the right, it is bounded by a crescent ligament, at the back - by the left part of the coronary and left triangular ligaments. This recess communicates with the lower, left subhepatic depression below.
The space under the visceral surface of the liver can be conditionally divided into two sections - the right and the left, the border between which can be considered a crescent and round ligament of the liver. The right subhepatic depression is located between the visceral surface of the right lobe of the liver and the transverse colon and its mesentery. Behind this depression is limited by the parietal peritoneum (hepatic-renal ligament, lig. Hepatorenale). The lateral right parietal depression is connected with the right circumcostal groove, in the depth through the gland opening - with the gland bag. The subhepatic space, located deep in front of the back edge of the liver, to the right of the vertebral column, is called the hepatic renal recess, recessus hepatorenalis.
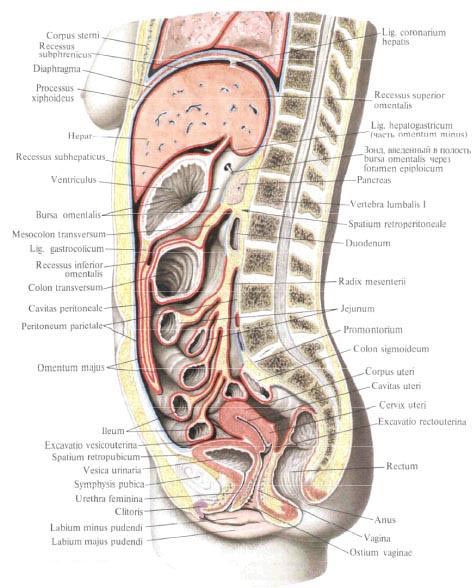
The left subhepatic groove is the gap between the small omentum and stomach on one side and the visceral surface of the left lobe of the liver on the other. Part of this space, located outside and somewhat behind the large curvature of the stomach, reaches the lower edge of the spleen.
Thus, the right sub-diaphragmatic and right subhepatic cavities surround the right lobe of the liver and the gallbladder (here the outer surface of the duodenum is facing). In topographic anatomy they are united under the name "hepatic bag". In the left sub-diaphragmatic and left subhepatic deepening, the left lobe of the liver, the small gland, the anterior surface of the stomach are located. In the topographic anatomy this department is called a pancreatic bag. The gland bag, bursa omentalis, is located behind the stomach. To the right it extends to the gland opening, to the left - to the spleen gates. The front wall of the stuffing box is a small omentum, the back wall of the stomach, the gastro-osseous ligament, and sometimes the upper section of the large omentum, if the descending and ascending sheets of the large omentum are not spliced and there is a gap between them, which is viewed as a continuation of the glandular bag down.
The back wall of the gland bag is the parietal peritoneum covering the organs located on the back wall of the abdominal cavity: the inferior vena cava, the abdominal aorta, the left adrenal gland, the upper end of the left kidney, the splenic vessels and below the body of the pancreas occupying the largest space of the posterior wall of the gland bag.
The top wall of the gland box is the caudate portion of the liver, the lower one is the transverse colon and its mesentery. The left wall is the gastro-splenic and diaphragm-splenic ligaments. The entrance to the bag is the gland opening, foramen epiploicum (omentale), located on the right side of the bag behind the hepatic-duodenal ligament. This hole is missing 1-2 fingers. Its anterior wall is the hepatic-duodenal ligament with the vessels located in it and the common bile duct. The posterior wall is the hepatic-renal ligament, behind which the lower hollow vein and the upper end of the right kidney are located. The lower wall forms the peritoneum, which passes from the kidney to the duodenum, the upper part - the tail portion of the liver. The narrowest section of the bag closest to the hole is called the vestibulum bursae omentalis; It is limited to the caudal lobe of the liver from the top and the upper part of the duodenum from below.
Behind the caudal lobe of the liver, between it and the medial pedicle of the diaphragm covered with the parietal peritoneum, there is a pocket - the upper glandular recess, recessus superior omentalis, which is open at the bottom towards the vestibule. The lower glandal recess, recessus inferior omentalis, is located from the vestibule, between the posterior wall of the stomach and the gastrointestinal ligament in front and the parietal peritoneal pancreas and mesentery of the transverse colon. To the left of the vestibule, the cavity of the omentum bag is narrowed by the gastropancreatic fold of the peritoneum, plica gastropancreatica, which extends from the upper edge of the glandular pancreas upward and to the left, to the small curvature of the stomach (it contains the left gastric artery, a gastrica sinistra). The extension of the lower depression to the left is the sinus located between the gastro-splenic ligament (front) and the diaphragm-splenic ligament (behind), which is called the splenic recess, recessus lienalis.
In the lower floor of the peritoneal cavity, on the back wall of it, there are two large mesenteric sinuses and two okolobobochno-intestinal furrows. Here, the bottom sheet of the mesentery of the transverse colon goes downward from the root to the parietal peritoneal sheet lining the posterior wall of the mesenteric sinuses.
The peritoneum, covering the back wall of the abdomen in the lower floor, passing to the small intestine, surrounds it from all sides (except the duodenum) and forms a mesentery of the small intestine, mesenterium. Mesentery of the small intestine is a double leaflet of the peritoneum. The mesentery root, radix mesenterii, runs obliquely from the level II of the lumbar vertebra to the left to the sacroiliac joint to the right (the place of the ileum into the blind). The length of the root is 16-18 cm, the width of the mesentery is 15-17 cm, but the latter is widened at the sites of the small intestine most remote from the posterior wall of the stomach. In its turn, the mesentery root crosses the ascending part of the duodenum at the top, then the abdominal aorta at the level of the IV lumbar vertebra, the lower vena cava and the right ureter. Along the root of the mesentery go, following from above from the left to the bottom and to the right, the superior mesenteric vessels; Mesenteric vessels give intestinal branches between the leaves of the mesentery to the wall of the intestine. In addition, between the leaves of the mesentery pass lymphatic vessels, nerves and located regional lymph nodes. All this is largely due to the fact that the duplicating plate of the mesentery of the small intestine becomes dense, thickened.
Mesentery of the small intestine peritoneal cavity of the lower floor is divided into two sections: the right and left mesenteric sinuses.
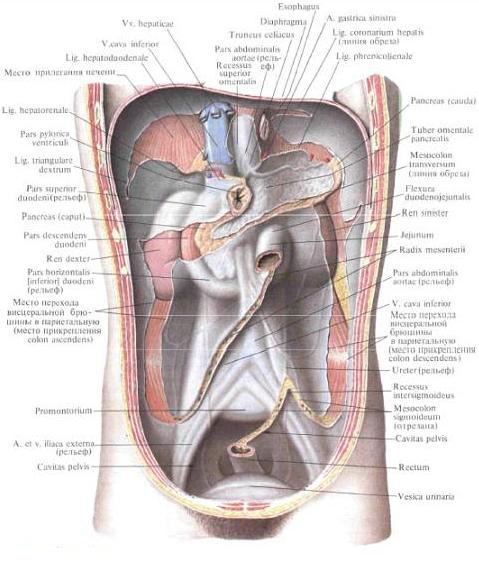
The right mesenteric sinus is bounded from above by the mesentery of the transverse colon, to the right by the ascending colon, to the left and from below by the mesentery of the small intestine. Thus, the right mesenteric sinus has the shape of a triangle, and is closed on all sides. Through the parietal peritoneum that lines it, the lower end of the right kidney (to the right) contours and shines above the mesentery colon; Adjacent to it is the lower part of the duodenum and the lower part of the head of the pancreas surrounded by it. Below in the right sinus is seen the descending right ureter and the ilio-colon artery with the vein.
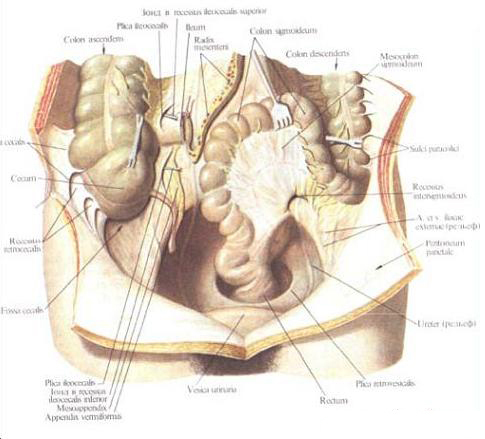
Below, in the place of confluence of the ileum in the blind, an ileocecal fold is formed, plica ileocecalis. It is located between the medial wall of the cecum, the anterior wall of the ileum and the parietal peritoneum, and also connects the medial wall of the cecum with the lower wall of the iliac top and the base of the appendix at the bottom. In front of the ileocecal angle there is a fold of the peritoneum - vascular cecal fold, plica cecalis vascularis, in the thickness of which the anterior cecal artery passes. The fold leaves from the front surface of the mesentery of the small intestine and approaches the anterior surface of the cecum. Between the upper edge of the appendix, the ileum and the wall of the medial portion of the bottom of the cecum is the mesentery of the appendix (appendix), mesoappendix. Feeding vessels pass through the mesentery, a. Et v. Appendiculares, and the regional lymph nodes and nerves are laid. Between the lateral margin of the bottom of the cecum and the parietal peritoneum of the iliac fossa are the cecal folds, plicae cecales.
Under the ileocecal fold lies the pockets located above and below the ileum: the upper and lower ileocecal depressions, recessus ileocecalis superior, recessus ileocecalis inferior. Sometimes under the bottom of the cecum there is a posterior cecal recess, recessus retrocecalis.
To the right of the ascending colon is the right circumcostal intestinal groove. It is bounded outside the parietal peritoneum of the lateral wall of the abdomen, to the left - by the ascending colon; Downward is reported with the iliac fossa and peritoneal cavity of the small pelvis. At the top, the furrow communicates with the right subhepatic and subdiaphragmatic depressions. In the course of the furrow, the parietal peritoneum forms transversely folded folds connecting the right bend of the colon with the lateral wall of the abdomen and the right diaphragmatic-ligament ligament, usually weakly expressed, sometimes absent.
The left mesenteric sinus is bounded from above by the mesentery of the transverse colon, to the left by the descending colon, to the right by the mesentery of the small intestine. The left mesenteric sinus communicates with the peritoneal cavity of the small pelvis. Sine has an irregular quadrangular shape and is downward open. The parietal peritoneum of the left mesenteric sinus is visible and contoured at the top - the lower half of the left kidney, lower and medially in front of the spine - the abdominal aorta and to the right - the lower hollow vein and the initial segments of the common iliac vessels. To the left of the spine, the left artery of the testicle (ovary), the left ureter and the branches of the inferior mesenteric artery and vein are visible. In the upper medial angle, around the beginning of the jejunum, the parietal peritoneum forms a fold that fringes the intestine on top and to the left; this is the upper duodenal fold (duodenal-neural fold), plica duodenalis superior (plica duodenojejunalis). To the left of it is a paroduodenal fold, plica paraduodenalis, which is a half-moon fold of the peritoneum, located at the level of the ascending part of the duodenum and covering the left colonic artery. This fold restricts the frontal non-constant paroduodenal recess, recessus paraduodenalis, whose posterior wall is the parietal peritoneum, and the lower duodenal fold (duodenal mesenteric fold), plica duodenalis inferior (plica duodenomesocolica), which is a triangular fold of the parietal peritoneum transient On the ascending part of the duodenum.
To the left of the root of the mesentery of the small intestine, behind the ascending part of the duodenum, is the pit of the peritoneum - the retro-duodenal depression, the recessus retroduodenalis, whose depth can vary. To the left of the descending colon is the left circumfiber intestinal groove; It is limited to the left (lateral) parietal peritoneum, lining the lateral wall of the abdomen. The groove passes to the ileum in the ileum and then into the pelvic cavity. Above, at the level of the left bend of the colon, the furrow is intersected by a constant and well-expressed diaphragmatic-fold pleat of the peritoneum.
Bottom between the bends of the mesentery of the sigmoid colon is the peritoneal intersigmoid depression, the recessus intersigmoideus.
You will be interested to read this:

Comments
When commenting on, remember that the content and tone of your message can hurt the feelings of real people, show respect and tolerance to your interlocutors even if you do not share their opinion, your behavior in the conditions of freedom of expression and anonymity provided by the Internet, changes Not only virtual, but also the real world. All comments are hidden from the index, spam is controlled.